The Journal
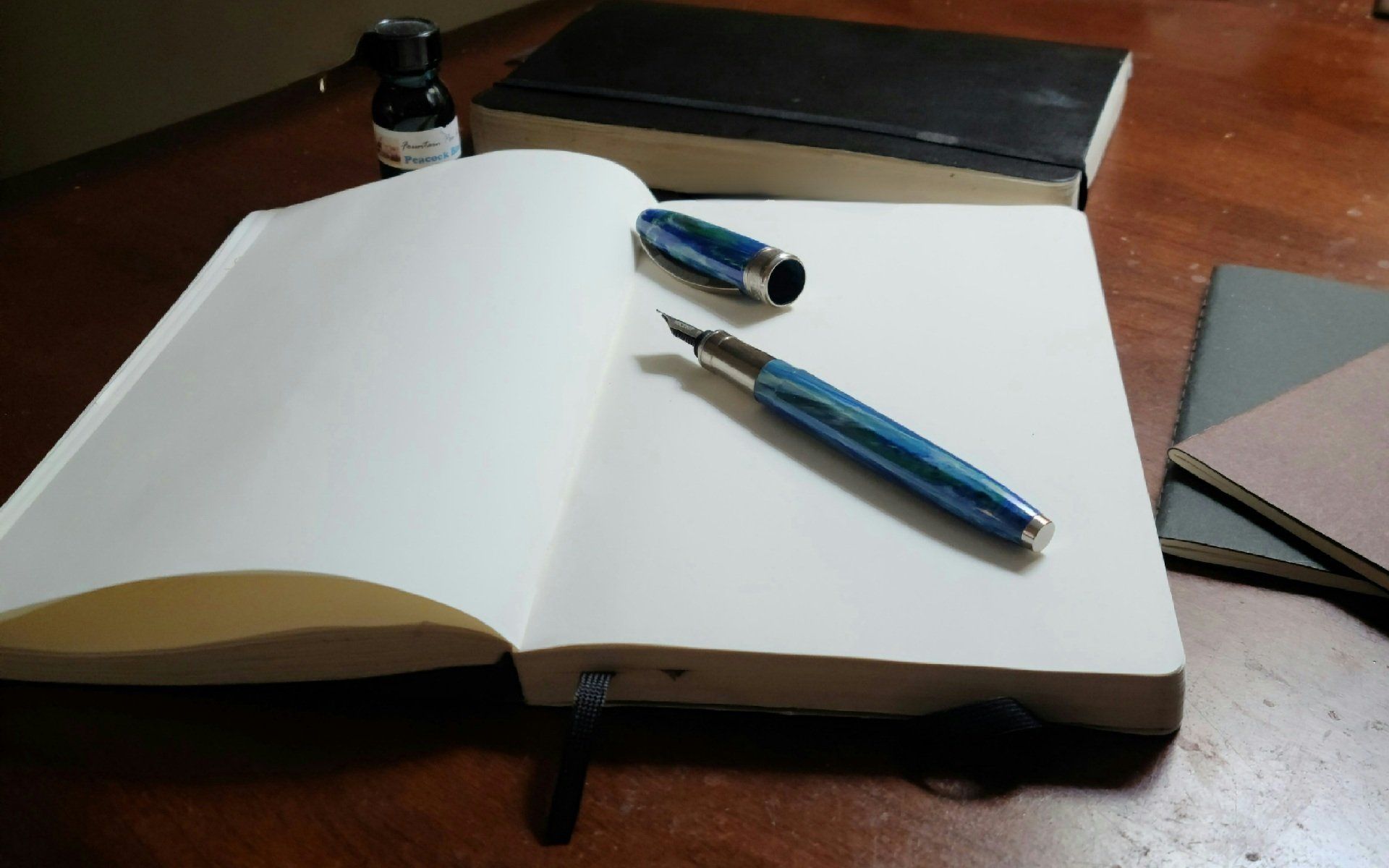
The journal itself may be simple or elaborate. You can use anything from sheets of paper to grade school notebooks to elaborately bound handmade paper diaries. Any writing instrument will do as well. I suggest a pen that provides clear lines. You can always create or embellish pages with images using a variety of colors, markers, and other writing instruments. My everyday writing instrument is a fountain pen which I’ve used for the last 20 years.
For you, as the occultist, you need a magickal record. To do that, here are suggestions for building your magickal journal. Following the experiments requires clear, concise, and complete documents. That record is for you to reflect and understand the work you do. However, a journal is more than just a recording. It allows you to capture all of the factors of your work. So we’ll create a series of prompts to help you remember the environment, your mood, the steps of the experiment, and everything that went into it.
Your journal may be as straightforward or as elaborate as you like. My recommendation is for you to use a paper journal. Writing enhancement memory and, like any other craft practice, encourages you to take more than you might with an electronic one. As a lifelong technologist, I love my gadgets and have copious electronic records. I choose to write rather than type because it allows me to be more expressive. However, don’t let that prevent you from using something that works for you. Electronic records are searchable; you can have both.
Your journal is separate from your BOS (Book of Shadows) or spell book you have acquired. Think of the magickal experience as an exercise in dining if your BOS or grimoire is the recipe book. The ritual or ceremony is the menu, the steps, and the spells that you put your magickal recipes into practice. The magickal journal is your Yelp review. 😊
I've included a sigil for your journal. It will provide focus and clarity of your writing.




